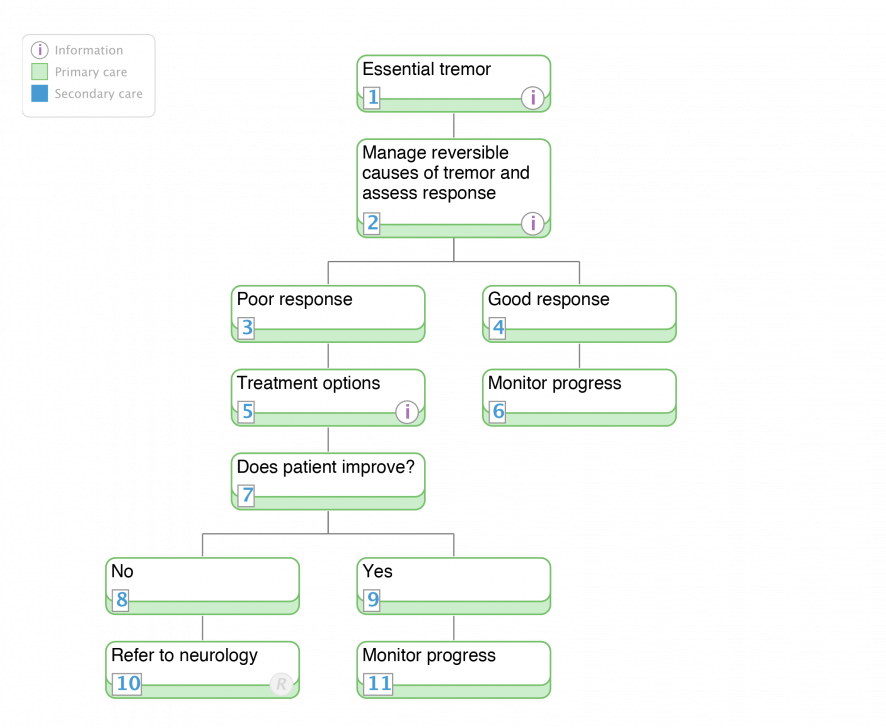
1. Essential tremor
Quick info:
Scope:
- this page provides specific information on the diagnosis and management considerations for essential tremor Definition:
- a largely symmetrical, postural or kinetic tremor involving hands and forearms that is visible and persistent. In some cases intention tremor may be present.
- It is one fo the most common and often mis-diagnosed movement disorders. The following should be excluded when making a diagnosis of essential tremor:
- other abnormal signs, especially dystonia (mild defects in gait are permissible in severe essential tremor)
- the presence of known causes of enhanced physiological tremor, including current or recent exposure to tremorgenic drugs or the presence of a drug withdrawal state
- historic or clinical evidence for a psychogenic origin of tremor
- convincing evidence of sudden onset or evidence of stepwise deterioration of tremor
- primary orthostatic tremor
- isolated voice tremor
- position-specific or task-specific tremors, including occupational tremors and primary writing tremors
- tongue or chin tremor
- leg tremor
- dystonic head tremor can present as an isolated head tremor but is considered by some as an essential head tremor Incidence and prevalence:
- the prevalence increases with advancing age
- the estimated prevalence is between 0.8-22% depending on the population studied
- typical features of essential tremor:
- a gradually progressive onset and course
- a positive family history in approximately 50% of cases
- essential tremor is alcohol responsive in approximately 50% of cases
- typically broadly symmetrical regular, postural and/or kinetic tremor of the hands
- in some cases an intention tremor is also present
- may cause impairment, disability and social handicap
- has a frequency range of 4-12Hz
- may be misdiagnosed as Parkinson's disease (see pathway). The latter should be considered when:
- typical unilateral onset of tremor in a hand and occasionally a leg
- a rest tremor, particularly a "pill rolling tremor" is present
- additional features are present:
- facial or vocal impassivity
- reduced arm swing on walking and shoulder shrug test
- cogwheel rigidity
- bradykinesia (slow movements with decrement)
- micrographia
- depression and cognitive changes may be present
- poor sense of smell
- other causes of parkinsonism and a dystonic tremor syndrome should be considered in the differential diagnosis of essential tremor
- investigation of essential tremor:
- routine haematology and biochemistry
- thyroid function tests
- copper studies (particularly if under 50 years at onset)
- protein electropheresis
- dopamine transporter (DAT) imaging if clinical difficulty in distinguishing essential tremor from Parkinson's disease. DAT imaging is usually normal in essential tremor and abnormal in Parkinson's disease
2. Manage reversible causes of tremor and assess response
Quick info:
The diagnosis of essential tremor should be suspended in the presence of known causes of enhanced physiological tremor until these are treated.
5. Treatment options
Quick info:
There is evidence based medicine data to support the use of the following treatments for essential tremor:
- Level A
- propanolol
- primidone
- propanolol long acting
- Level B
- atenolol
- sotalol
- topiramate
- gabapentin
- alprazolam
- Level C
- clonazepam
- clozapine (beware of agranulocytosis, which can be fatal)
- nadolol
- nimodipine
- botulinum toxin A
In essential tremor there is evidence based medicine data to support the use of:
- For head tremor:
- Level B: propanolol
- Level C: botulinum toxin A
In patients with disabling essential tremor that is refractory to medical treatment stereotactic surgery should be considered:
- thalamotomy (level C)
- Thalamic stimulation (deep brain stimulation) (level C)
- 60-90% decrease in tremor (assessed by clinical rating scale)
- deep brain stimulation has fewer adverse events than thalamotomy (level B)
- bilateral thalamotomy is not recommended (Level C)
- this is because of a high incidence of speech disorders associated with bilateral thalamotomy
References
Zesiewicz TA, Elble R, Louis ED. Practice parameter: therapies for essential tremor: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2005; 64: 2008-20.
Ferreira J, Sampaio C. Essential tremor. Clin Evid 2005; 1608-21.